

Treatment of diffuse large B-cell lymphoma (DLBCL) in patients over the age of 80 years is challenging due to existing comorbidities and frailty in the face of an aggressive disease. Standard chemo-immunotherapy can sometimes be difficult to administer to these patients due to toxicities, requiring dose adjustments and interruptions. There are no definitive guidelines to help direct therapy in these patients and treatment decisions are often subjective.
The objective of this study was to retrospectively review treatment patterns and outcomes of DLBCL in patients over the age of 80 years. All patients who were referred to the Tom Baker Cancer Centre in Calgary, Alberta from 2012-2017 were retrospectively reviewed. Data collected included patient characteristics, comorbidities that were used to calculate the Charlson Comorbidity Index (CCI), revised International Prognostic Index (IPI), chemotherapy regimen(s), dose reductions and interruptions, and mortality. The primary outcome was overall survival (OS).
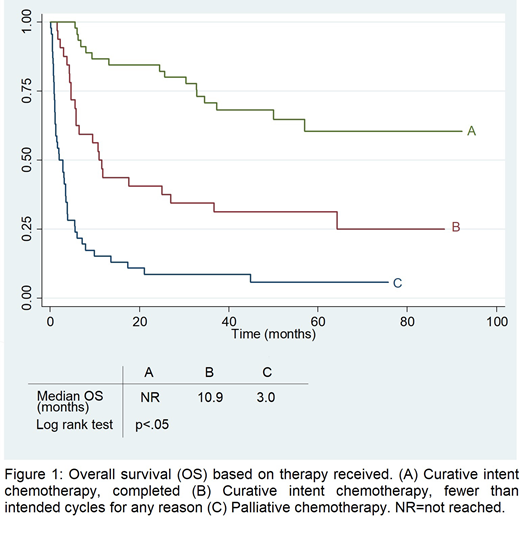
A total of 123 patients with DLBCL over the age of 80 were referred to the cancer center at diagnosis. The average age was 84.9 years (IQR 82-87.5). At diagnosis, 62.3% of patients had an ECOG≥2 and 65.8% of patients had an IPI greater than 3. The most common comorbidities described were a history of congestive heart failure (20%), diabetes (16%) and MI (20%). Patients received either curative intent chemotherapy (62.6%) or palliative therapy (37.4%). The curative intent chemotherapy regimens included dose-reduced R-CHOP (31.5%), full dose R-CHOP (11.8%), R-CEOP (14.2%), and other chemotherapy regimens (3.9%). Palliative therapy included PEP-C chemotherapy (4.7%) or treatment with steroids (13.4%) or no treatment at all (20.5%). There were 28 patients (22.7%) who received adjunctive radiotherapy for limited stage or bulky disease. Risk factors at diagnosis for mortality included elevated LDH (OR 3.14, CI 1.42-6.93, p<0.05) and ECOG≥2 (OR 2.15, 0.99-4.67, p<0.05). Every 1 point increase in patients' CCI at diagnosis was associated with an increased risk of death (OR 1.38, 95% CI 1.05-1.82, p=0.02). The cumulative OS at 2 years was 44.7%. Patients who received any amount of curative intent chemotherapy did better than the palliative group (See Figure 1). Within the chemotherapy group, 33.3% of patients stopped their treatment early. These patients had better survival than the palliation group (HR 0.56, 95% CI 0.34-0.94, p=0.04) but overall still had a poor prognosis with a median OS of 10.9 months.
Very elderly patients with DLBCL still remain a very challenging population to treat with most patients presenting with high risk disease and poor functional status. Without chemotherapy, the overall prognosis is dismal. Patients who are able to complete treatment with chemo-immunotherapy have the best survival despite the risk of toxicities associated with more intensive treatment but that survival is significantly shortened if they are unable to complete their planned cycles.
Owen:AbbVie, F. Hoffmann-La Roche, Janssen, Astrazeneca, Merck, Servier, Novartis, Teva: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal